33 Antihypertensives
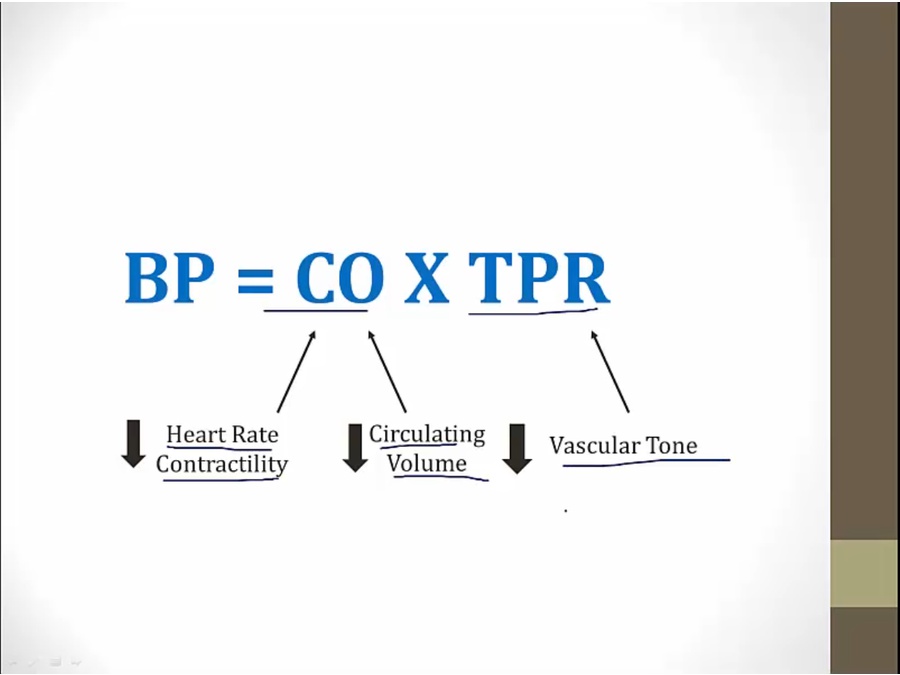
- antihypertensives work by either decreasing CO or decrease TPR
Beta Blockers
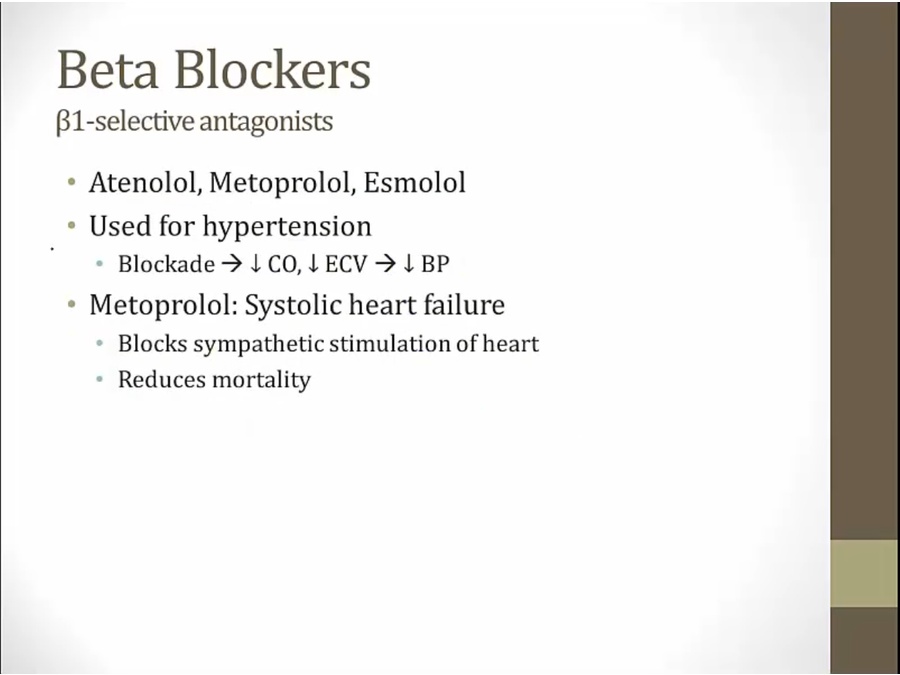
- not really used for hypertension
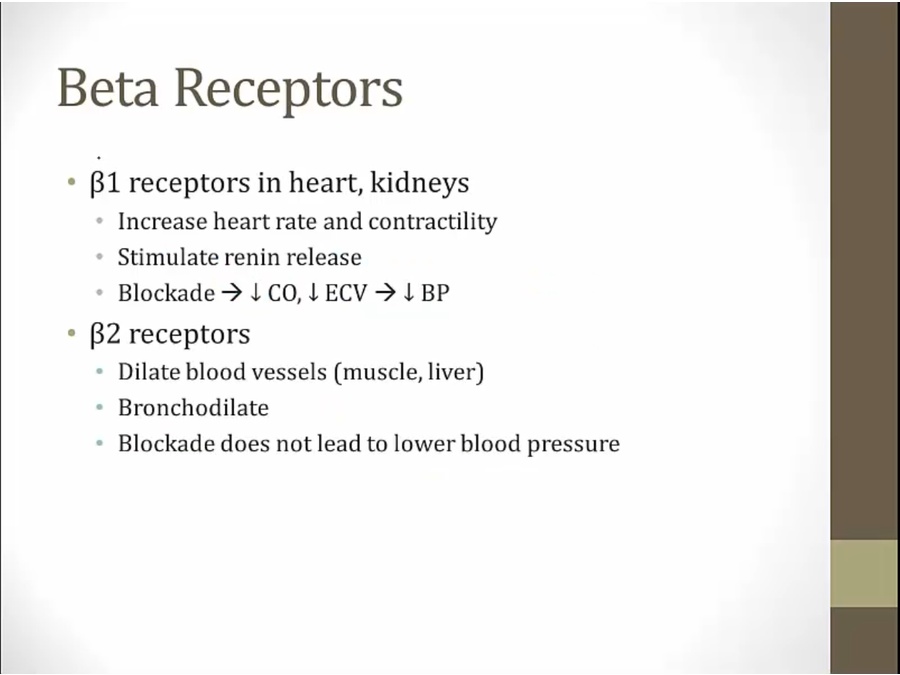
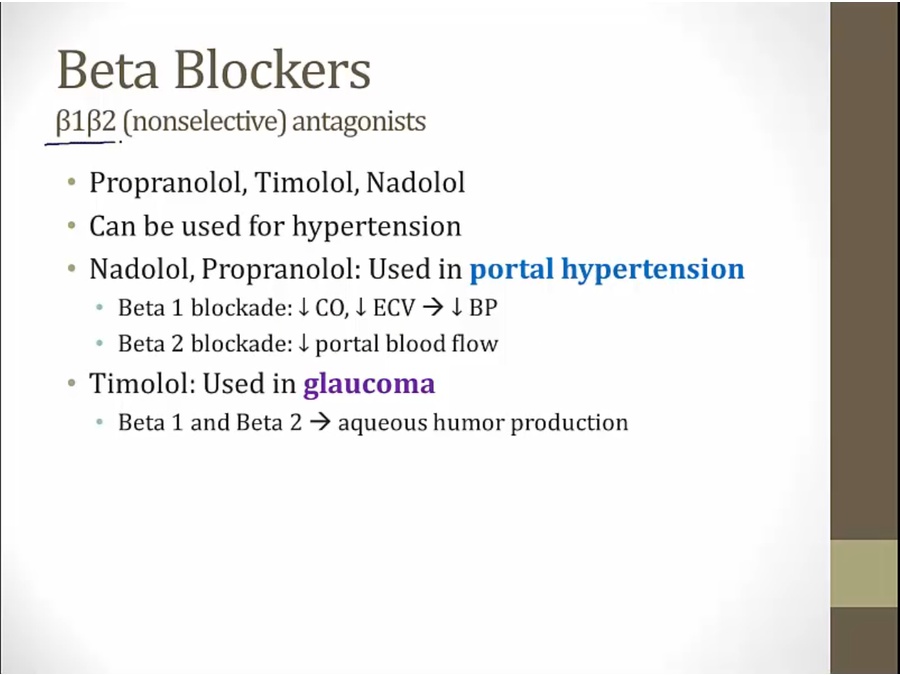
- b1 blockade: general lower BP, including portal system
- b2 increase flow to liver, block to decrease flow
- carvedilol: clinical trial shows benefit, not because of special receptor
- at low sympathetic level, higher activation of beta receptor than sympathetic activity, thus agonist
- high level, lower activation of beta receptor than sympathetic, thus blocker
- fatigue, etc: blunt CNS activity
- hyperlipidemia not clinically relevant
- given because many benefits
- diabetics often hypoglycemic because taking insulin
- BB cause hypoglycemia and masks symptoms, except sweating (Ach receptors)
- decompensated
- acute HF: pt with pulmonary edema/sick from HF can get very sick with BB's lowering of CO
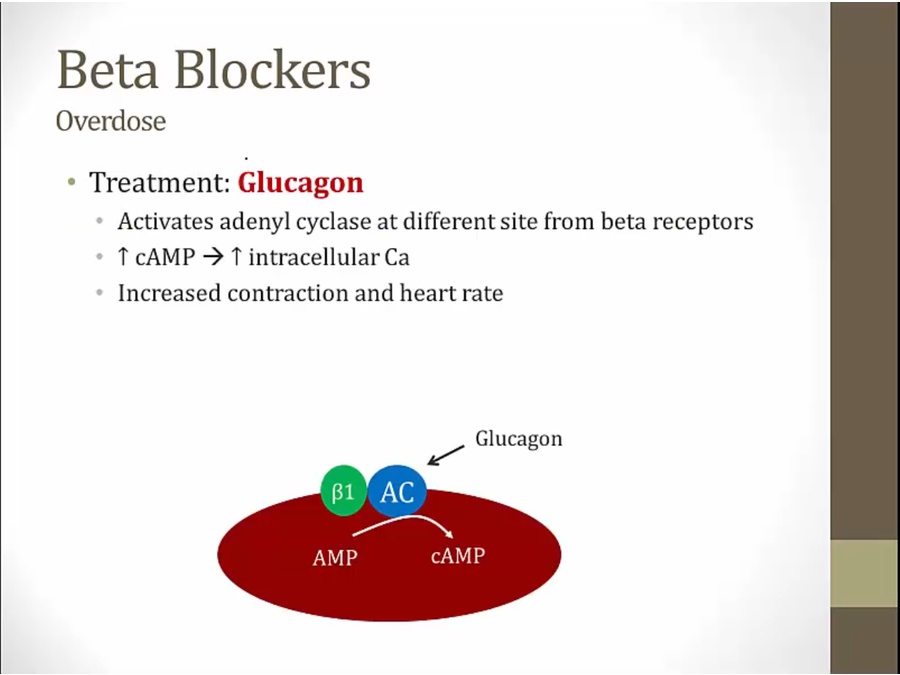
- stimulates myocardiocytes at different site
- stimulate heart and bypass beta receptors
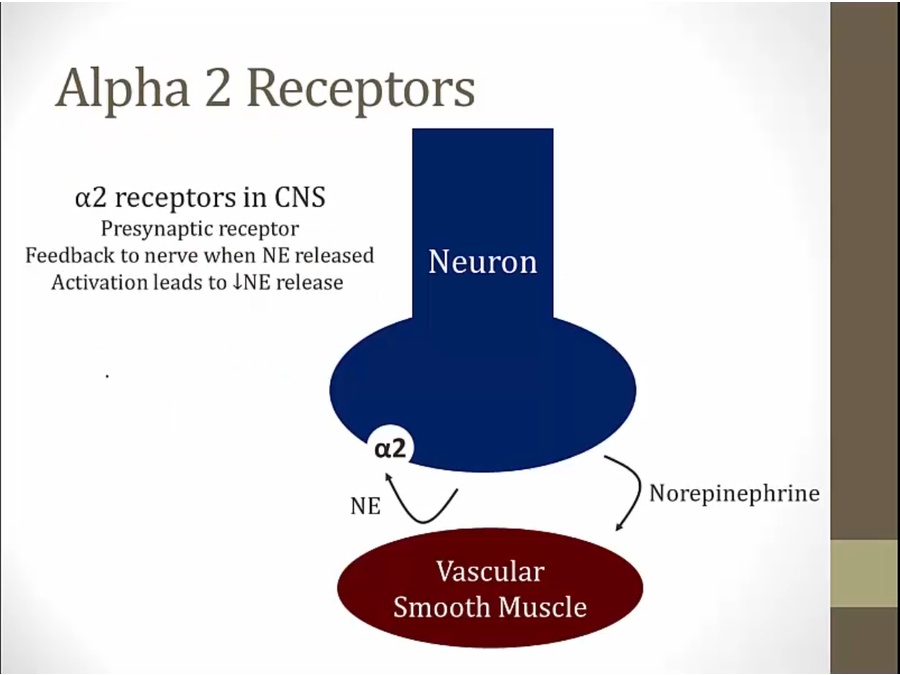
Alpha Drugs
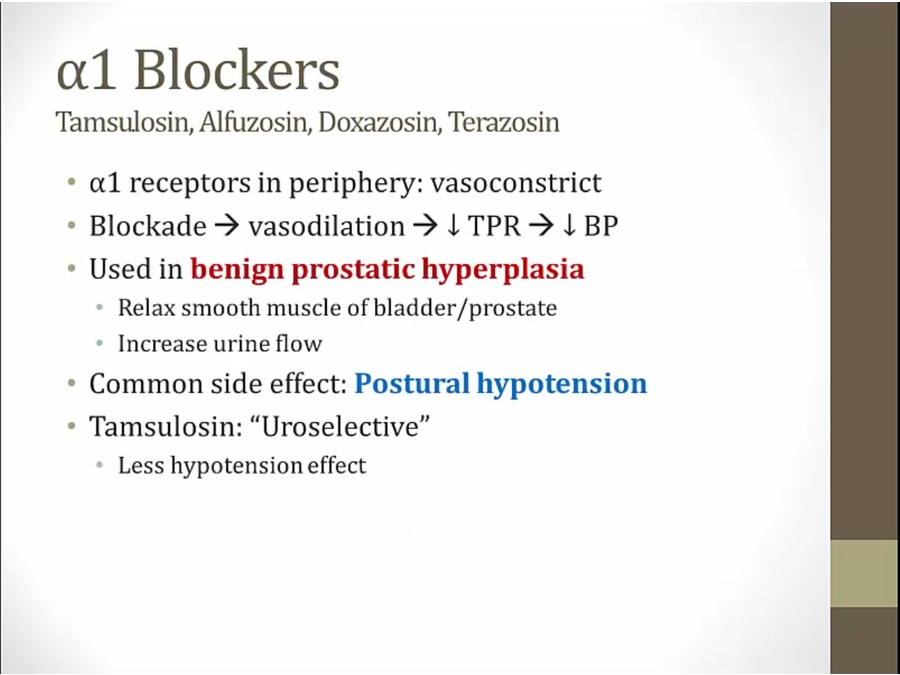
- tamsulosin very good for BPH
- warm autoimmune hemolytic anemia
CCB
Dihydropyridines
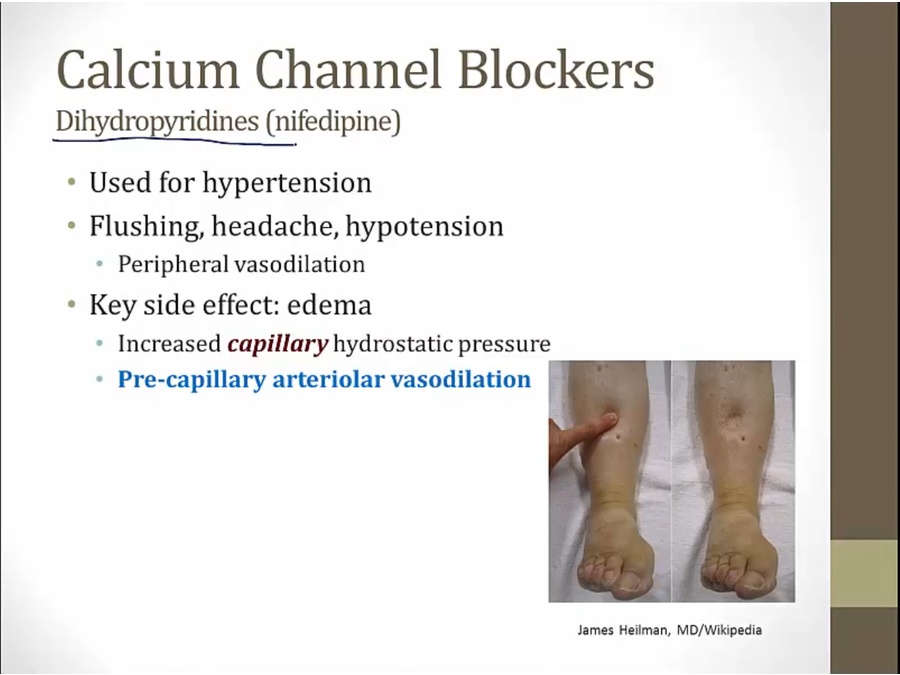
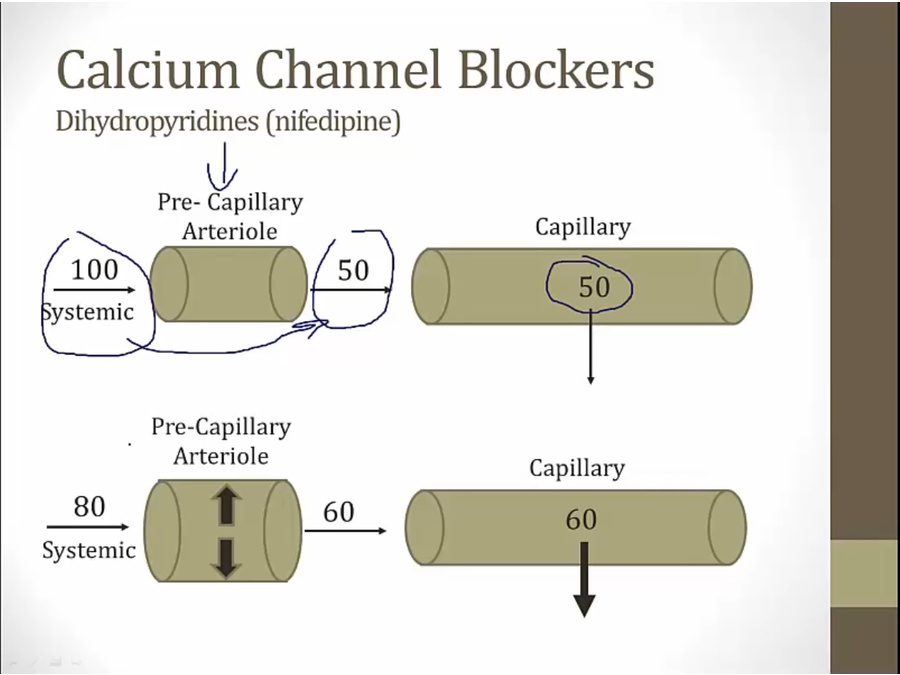
- pt not taking CCB: arteriole constrict, leading to lower hydrostatic pressure in capillaries
- CCB: dilate arteriole, higher hydrostatic pressure
- like b1, slow HR, decrease contractility
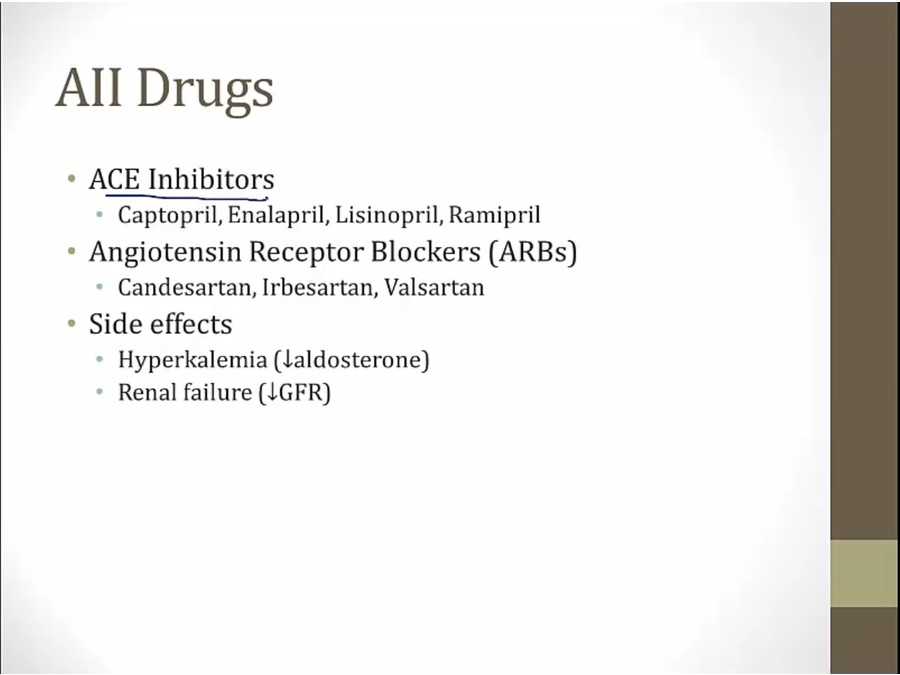
AII
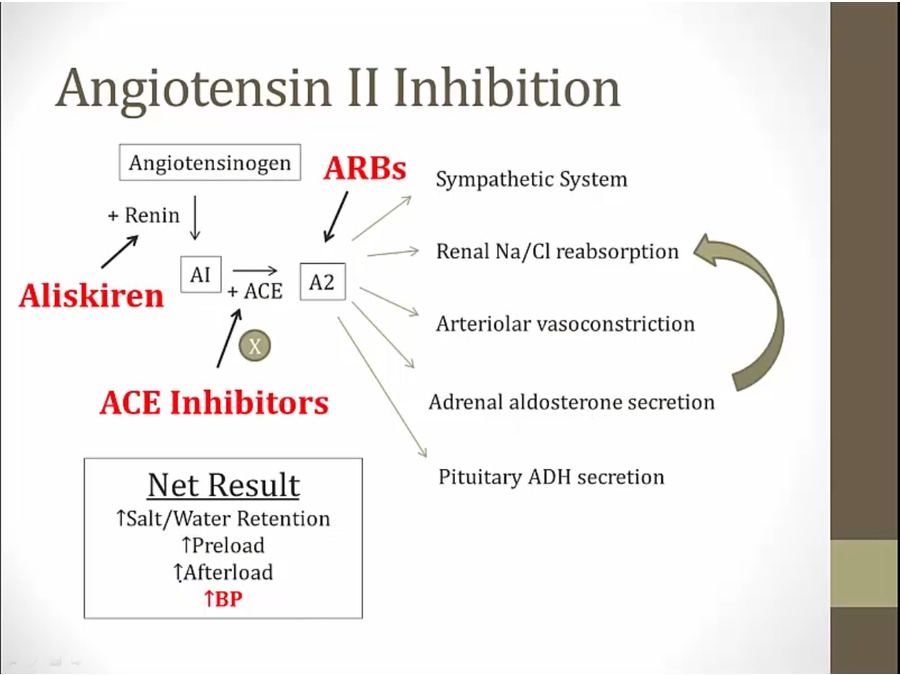
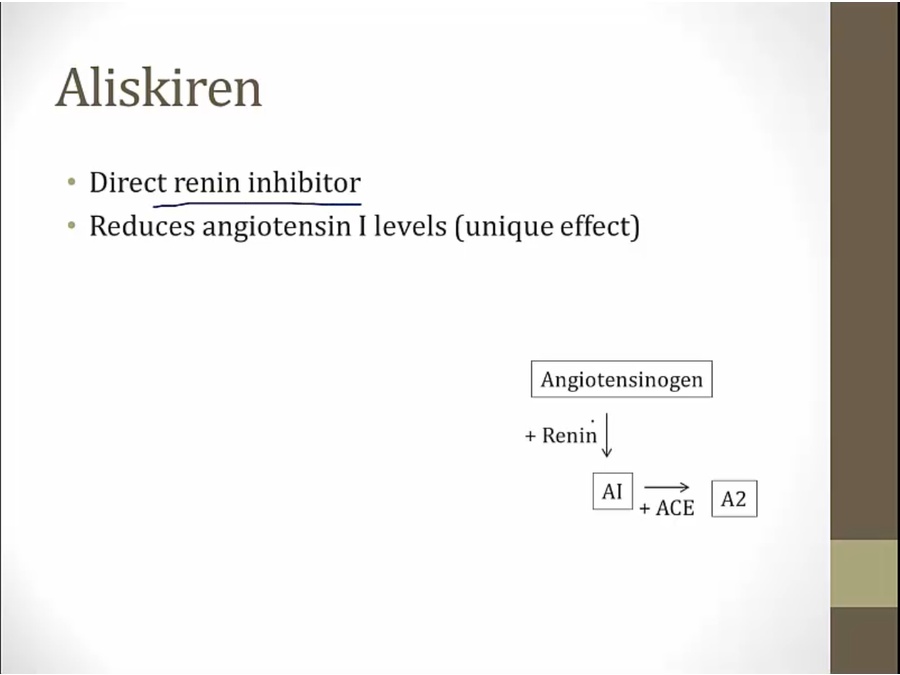
- inhibits renin, decrease AI production
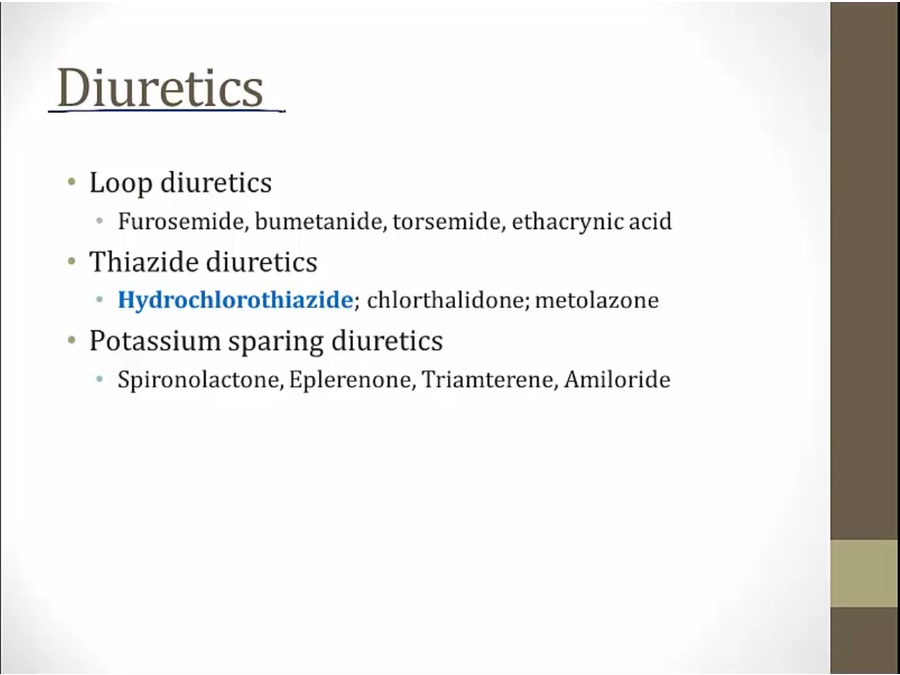
- HCTZ: used often for antihypertensives by inhibit Na absorption
Hydralazine
Hypertensive Emergency
- rapid acting drugs that can be titrated carefully
- increased renal perfusion
Antihypertensive SE
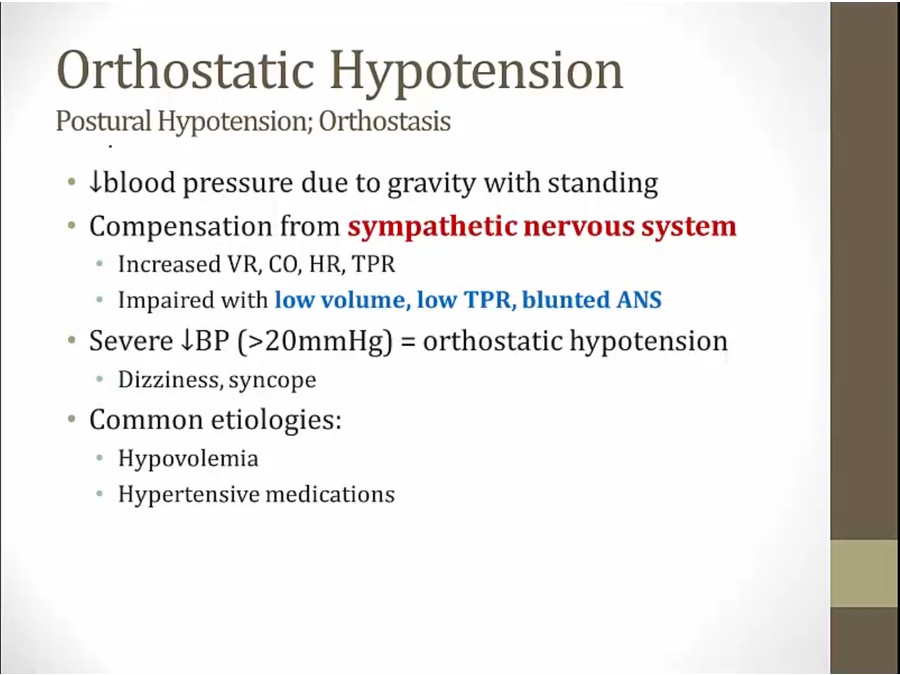
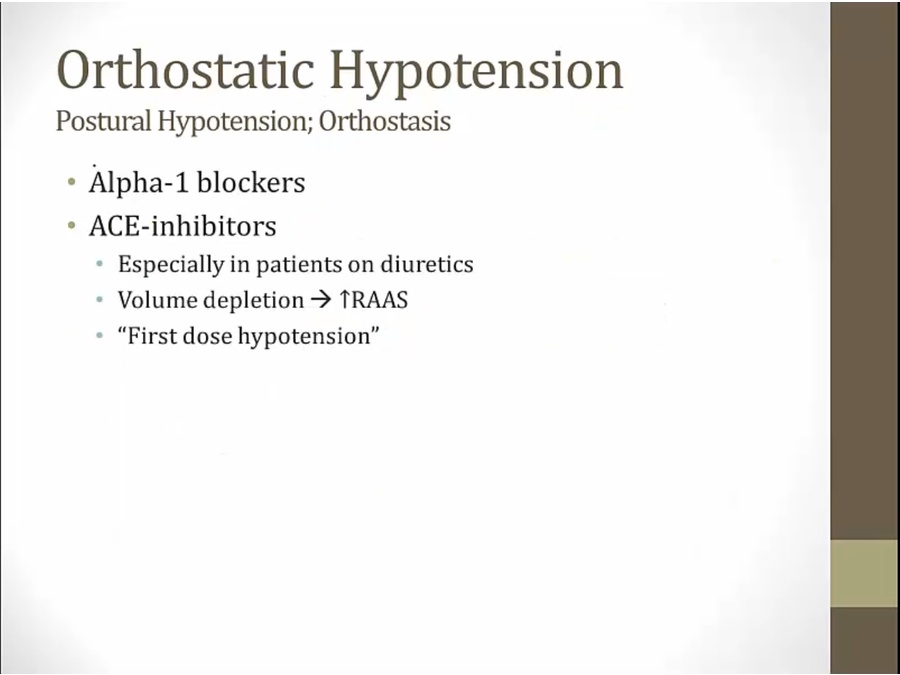
- diuretic pts: dependent on AII to maintain BP
- ACE I block AII
- occurs with first dose of ACE I given to diuretic pt
Choosing Antihypertensives
- RAAS blockade leads to malformation
- ACE I: decrease AII, renal failure
- aldosterone decrease: more K
Backlinks